
Overview
This graduate research and design project aimed to address the challenges of diabetes management in rural Texas, where resources are limited, medication cost is high, and diabetes education resources are scarce. Based on several types of research, we developed a four-point strategic plan that would set the groundwork for future efforts in establishing an array of web- and community-based resources.
My Roles and Responsibilities
I was one of 11 team members. And while I made varying contributions to each subteam (research, multimedia, content, etc.), I did lead the web subteam.
Supporting research team
Through performing a literature review, competitive analysis, and heuristic evaluation, I contributed to additional research.
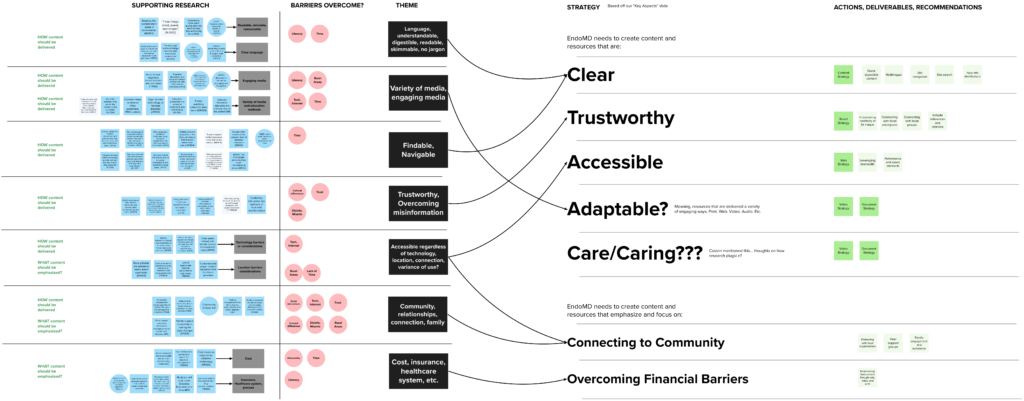
Translating research insights into strategy
Leveraging research insights, I authored the service design-based strategic framework that would guide the entire project.
Leading web strategy
While leading the web team, I directed all usability, accessibility, heuristic, and structural recommendations for the web portion of this project.
Rebuilding information architecture
I audited the previous website structure and designed a new information architecture based on research insights and overall strategy.
View full list of team members
EndoMD Team
The team consisted primarily of 11 UNT interaction design graduate students, two UNT professors, and our primary client/stakeholder.
Lydia B.
Multimedia lead
Aqsa C.
Content lead and research
Giselle E.
Research lead
Fatima H.
Research
Rebekah I.
Research and content
JiYun K.
Research and web
Sushma K.
Multimedia lead
Kendrick M.
Project lead
Luis Merino (me)
Web lead
Bansri S.
Research and web
Christina T.
Visual branding lead
Michael Gibson
UNT Professor
Cassini Nazir
UNT Professor
Dr. Wasim Haque
Client/Stakeholder
Background
EndoMD.com, created by Dr. Wasim Haque, was an educational resource aimed at informing patients and colleagues about diabetes risks and management. Dr. Haque sought to expand his outreach to patients, especially elderly rural Texans. We would dig into the problem and make research-backed recommendations for the future of EndoMD.
Here is what we knew about the experience of rural diabetic patients:
Resources are limited. Human resources, such as physicians or healthcare providers, are limited. In Denton county, one primary care physician is demanded to provide services to 1,721 patients.
Cost of medications is high. The financial toll that diabetes management takes on lower-income patients distracts them from taking their medications on a regular basis.
Lack of understanding. The failure of the healthcare provider and patients to understand it is a progressive disease. In many cases, it is not the patient’s fault that patients are not able to control their diabetes. They are doing what they can do.
Part 1
Discovery
Our first tasks were to dig into the topic of diabetes and begin to frame the problem we would be solving. As a team, we engaged in the following activities:
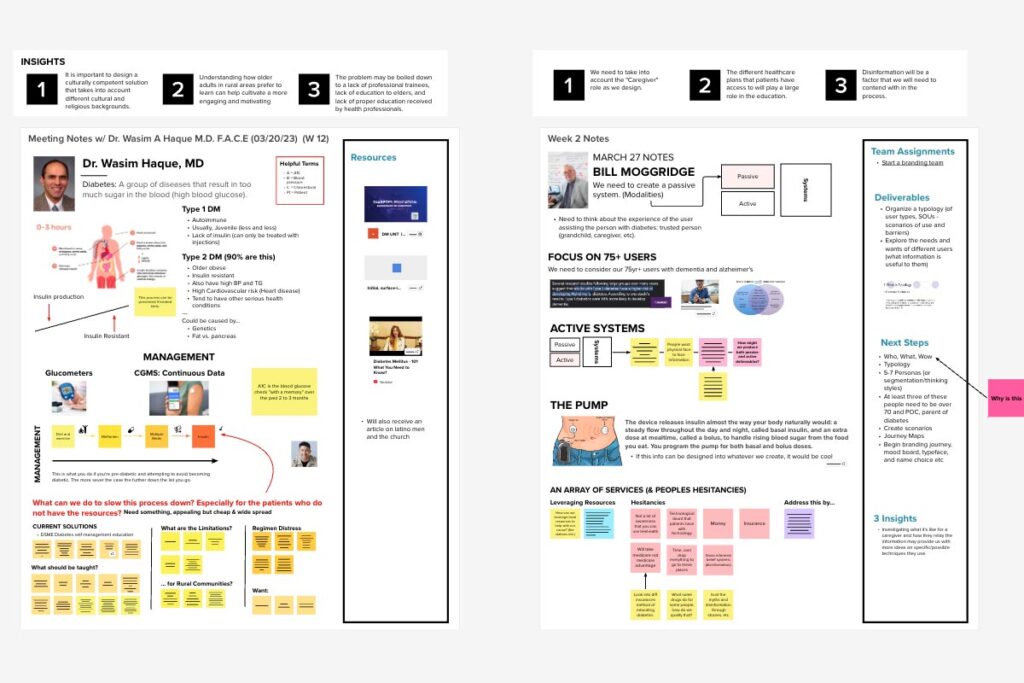
Stakeholder meetings
We met several times with Dr. Haque and his team to better understand the medical importance of diabetes and establish goals and direction for the project.
Topics learned were:
- Diabetes 1 and 2 basics
- Diabetes distress
- Known challenges
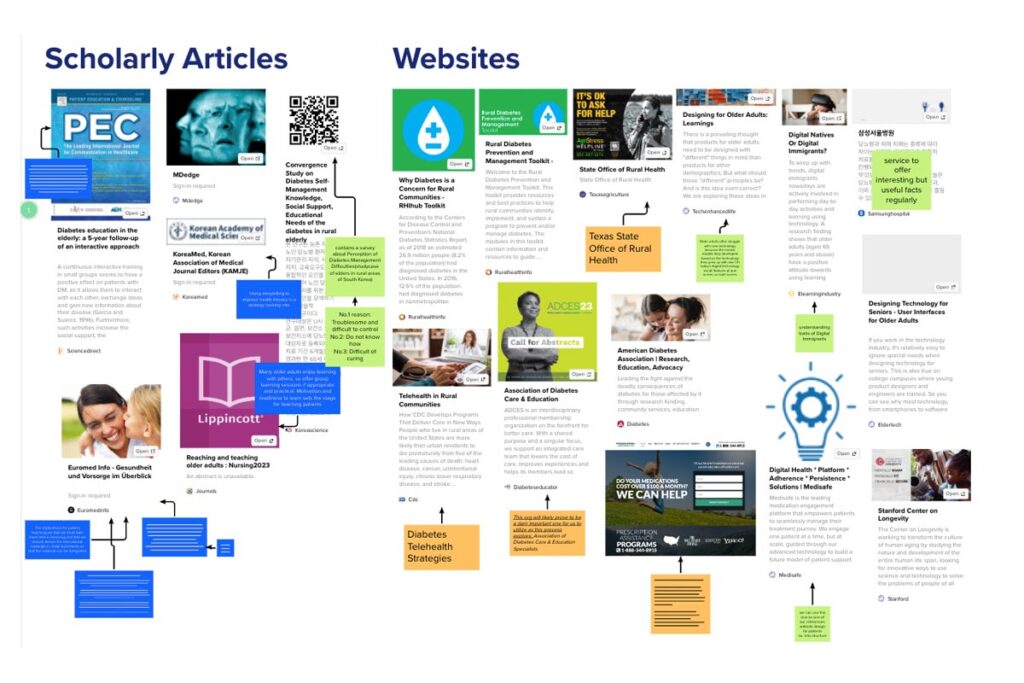
Literature review
From our stakeholder meetings, we knew there were many topics to unpack including senior medical care, diabetes distress, the rural experience, telehealth, and misinformation.
An example included:
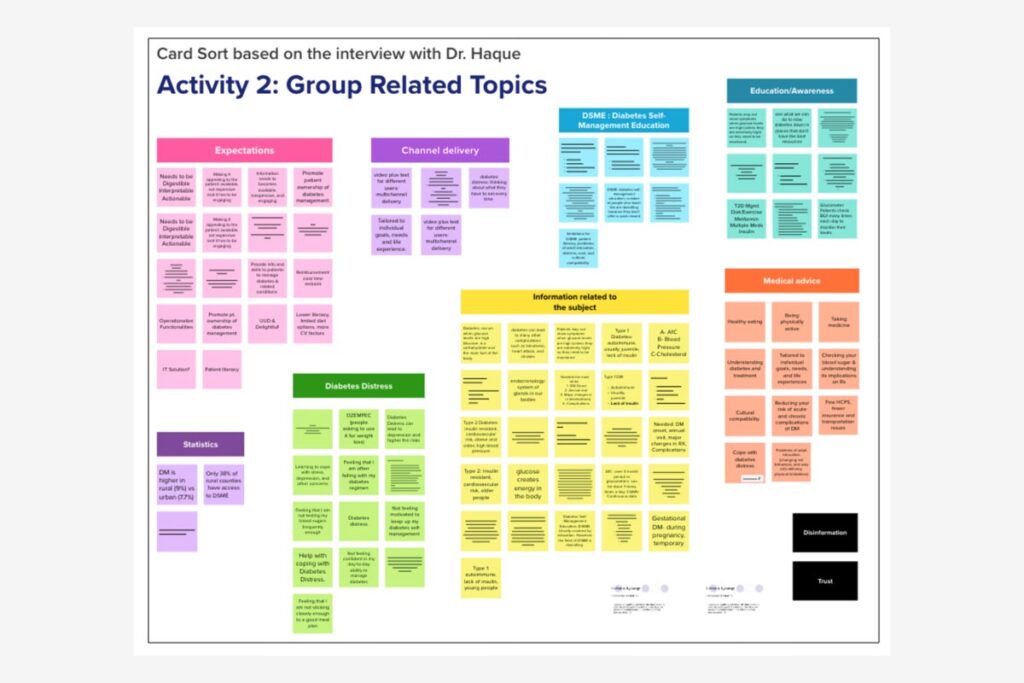
Affinity mapping
We aggregated insights and takeaways from our stakeholder meetings and literature reviews on digital stickies. In an online workshop, we used affinity mapping to create groupings or themes. Some of these included:
- Diabetes distress
- Medical advice
- Expectations in proposed solutions
My Responsibility
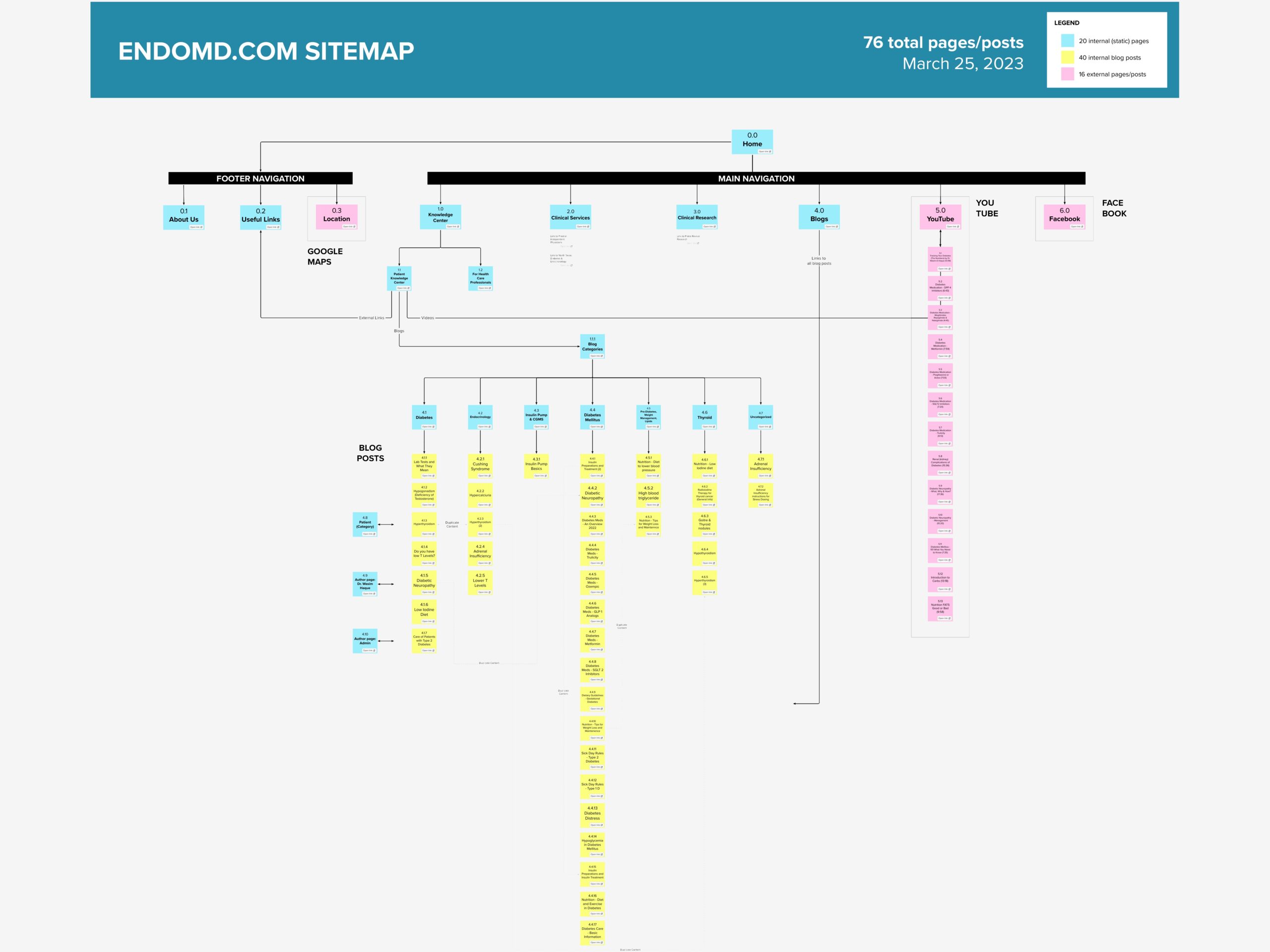
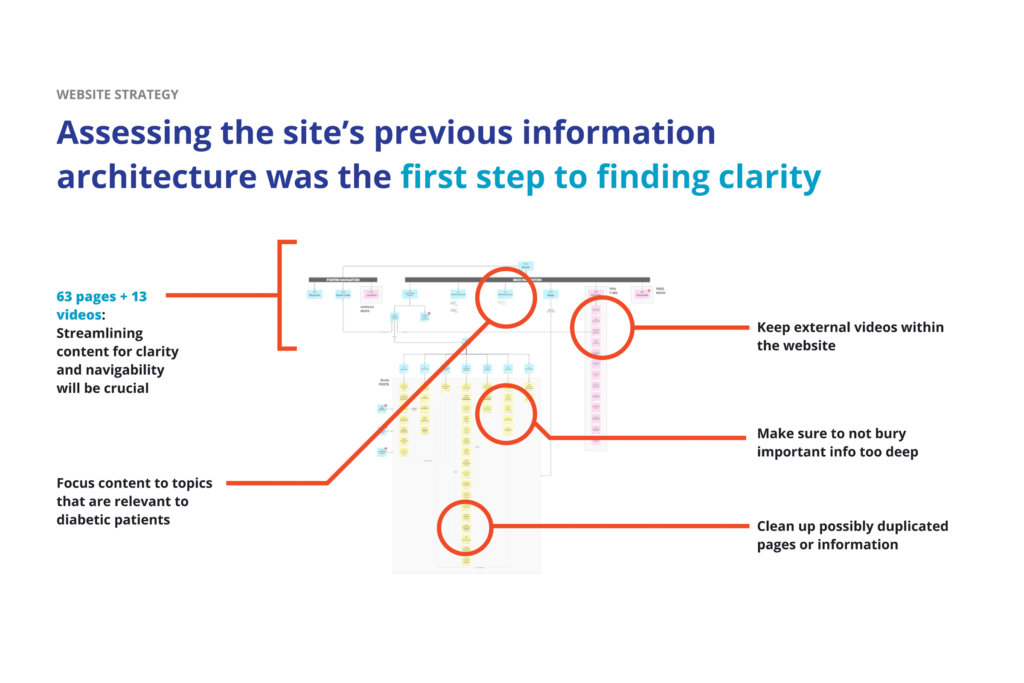
Information architecture audit
I mapped out the existing architecture of the EndoMD website to visually understand its structure and flow:
- 76 total pages
- 40 internal pages and articles
- 16 external pages and content
The website navigation indicated there were three main sections, but upon close review of the sitemap, the bulk of the website content was the repository of blog posts under the “Knowledge Center” section. This showed an uneven structure.
I also discovered that this content was buried three levels of pages and that there were a handful of duplicate pages.
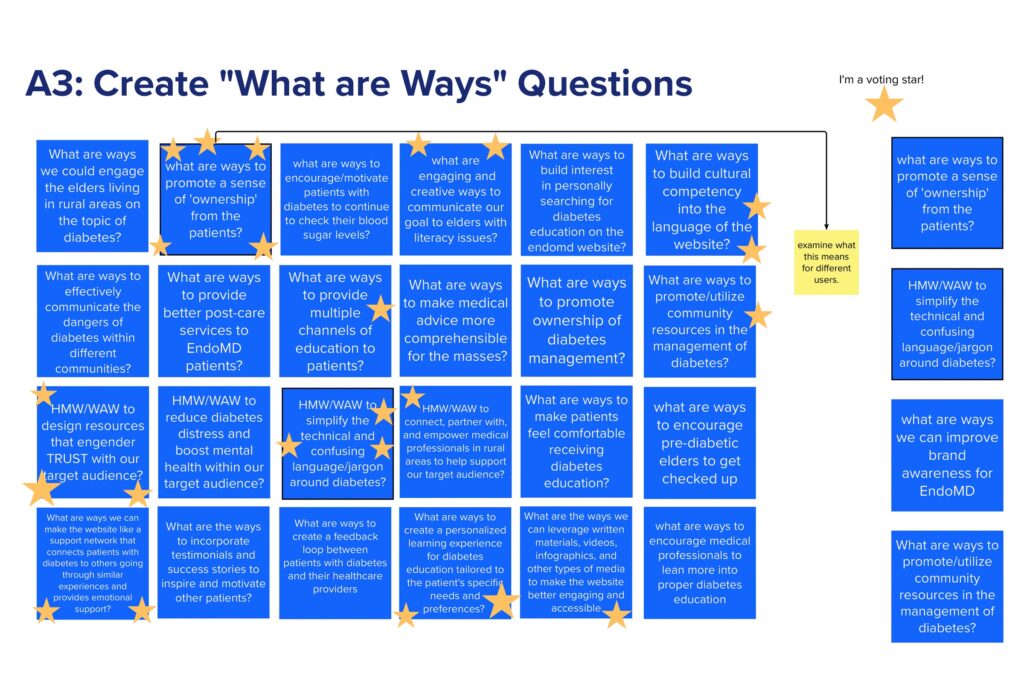
“What Are Ways”
The team also performed a “What Are Ways” activity to do some early-stage ideation on solution approaches. The top ranked ideas were:
- Promote a sense of ownership within patients
- Simplify the confusing jargon around diabetes
- Utilize community resources in the management of diabetes
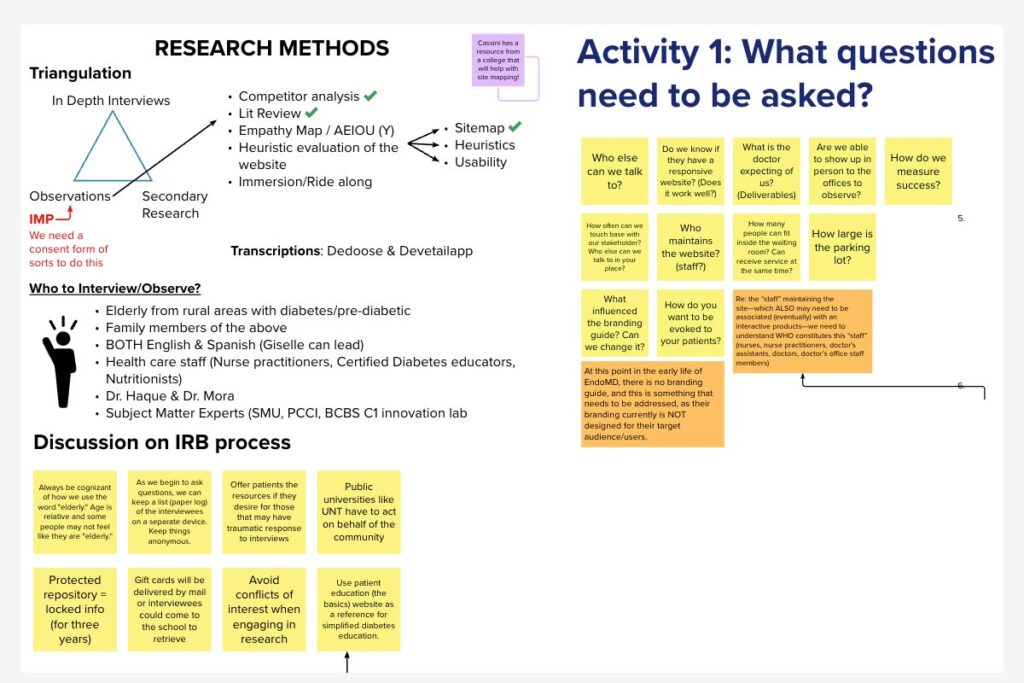
Research preparation
We aggregated questions that we knew we needed to ask actual diabetics patients and educators. We also developed a plan for research triangulation which included a mix of methods:
- In-depth interviews
- Usability testing
- Observations
- Literature reviews
- Competitor/collaborator analysis
- Heuristic evaluation
Formation of subteams
Based on all our discovery activities, we know that branding, research, website, multimedia and content needed to be focus areas in the remainder of the project. So we formed subteams around these needs.
See a full listing of all team members in the overview section.
Our Problem Statement
We aim to investigate the communication channels that exist for pre-diabetes and diabetes patients by interviewing multiple stakeholders and exploring best practices in order to create a more engaging and comprehensible medical resource.

Part 2
Research
The research team conducted over nine interviews and eight usability tests with diabetic patients, educators, and experts to understand the challenges being faced by the rural Texas community.
Research Methods
In-depth Interviews
Research team conducted six interviews with people living with diabetes from Texas and three interviews with healthcare professionals
Observations
- “Am I really taking the best medication for me? I could Google it, but would I even trust it?”
- “[Diabetes] affects literally every single aspect. It changes everything.”
- About rural life: “Driving is nothing. 40 minutes. An hour.”
Usability Testing
Research team directed eight usability tests with older adults on existing EndoMD and similar websites. All participants were 40 or older.
Observations
- “I like things short, sweet, and simple.”
- “I would expect to find keywords in the title of the videos.”
- “One thing that helps people with diabetes is to know that other people are also going through it.”
My Responsibility
Heuristic Evaluation
Using the rubric from Kate Finn’s and Jeff Johnson’s book “Designing User Interfaces for an Aging Population,” I performed a heuristic evaluation on the existing website.
Takeaways & Recommendations
- Language in articles were too technical. Copy should be written at a third grade level.
- It would take four clicks to get into blog info. Site hierarchies should be shallow.
- There was insufficient color contrast on some text.
- Site was using animations. Animated graphics are not relevant and create unnecessary distraction.
Research Insights
The following eight insights were distilled from all primary and secondary research methods performed by the entire team.
Community is essential
Healthcare systems fail diabetic patients
Diabetes education is not standardized
Misinformation causes a lack of trust
Language should be digestible by all
Information should be easy to find
Testimonials build trust
All screens should be responsive

Part 3
Building a Strategy
The next step was to build strategic planks, or what we were calling strategic “building blocks.”
Reviewing all research insights, takeaways, and known barriers, we mapped out what these five building blocks would be:
The Five Strategic Building Blocks
These building blocks would support each one of our recommended channels and would be weaved throughout the remainder of this project.
Educate
Provide comprehensible information to inform and enhance the quality of life for diabetics.
Clarify
Enhance the dialogue with the patient so that communications are more clear and concise.
Encompass
Support social inclusion for people with disabilities, older adults, and people in rural areas.
Build Trust
Strengthen the relationship with each patient
by providing relevant information for them.
Care With Empathy
Understand the personal experience and various needs of the patient.
My Contribution
The Engagement Model & an “Array of Services”
Armed with research and insight, our team fully came to the conclusion that our recommended solution should be an array of services. Using service design thinking as a framework, I ideated on possible approaches to implementing this “array of services.”
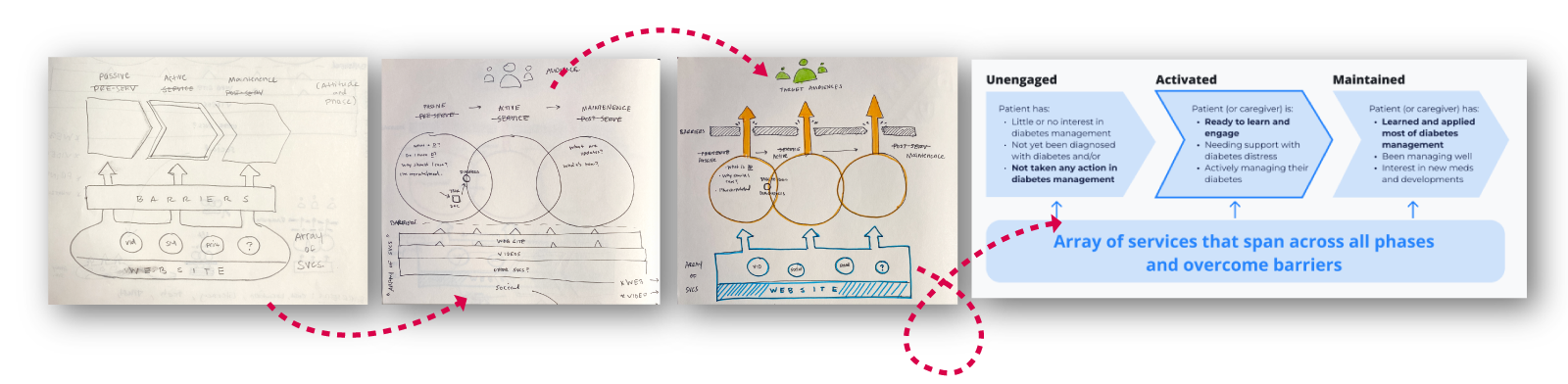

The array of services would span across all phases of a person’s journey with diabetes and push them to overcome the barriers they face. We would recommend services designed to move patients toward action and engagement.
Part 4
Web Strategy
I led the development of the remainder of our web strategy, based off these building blocks:
Educate
Thanks to the knowledge and resources offered through the website, our audience can become empowered and confident enough to further engage in their own diabetes care.
Clarify
Our audience has a hard time reading long paragraphs of technical English, because it might be their second language. To maximize their ability to learn, the website will feature resources that are clear, understandable, and easy to find.
Encompass
Our audience’s only access to the internet might be on their 10-year-old smartphone and only when they’re in-town. So, the website will be navigable and usable on slow-speed mobile devices.
The Process
Old sitemap analyzed
The first step to finding clarity was analyzing the site’s previous IA. Navigation, content, video embeds, and hierarchy were all things that needed to be addressed.
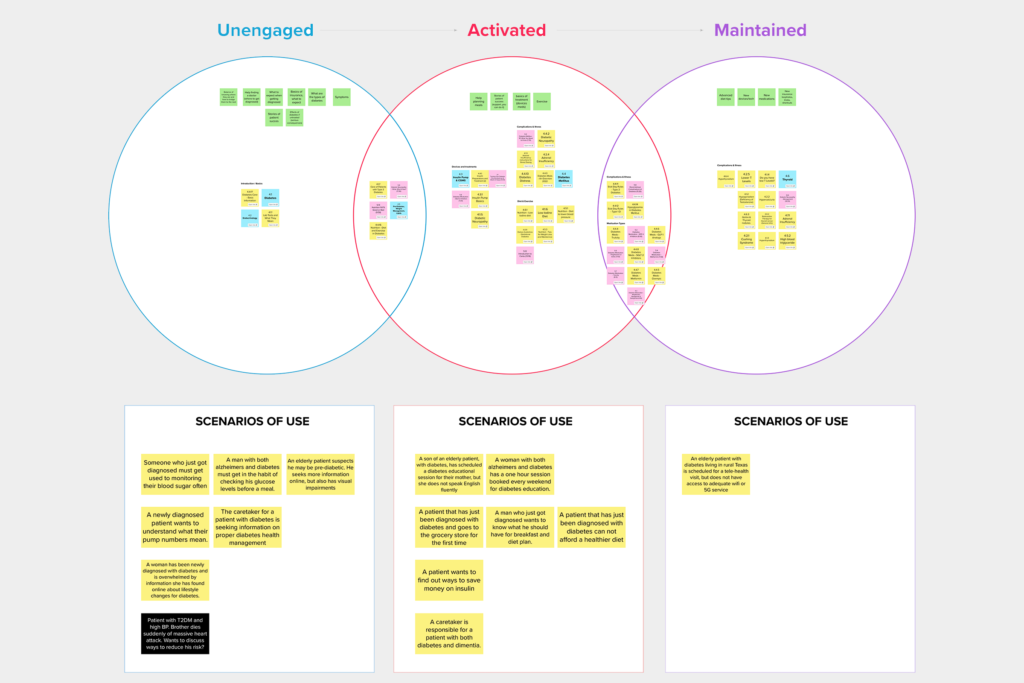
Aligning IA to strategy
We organized existing content by engagement phase methodology: unengaged, activated, and maintained. We also created scenarios of use for each phase.
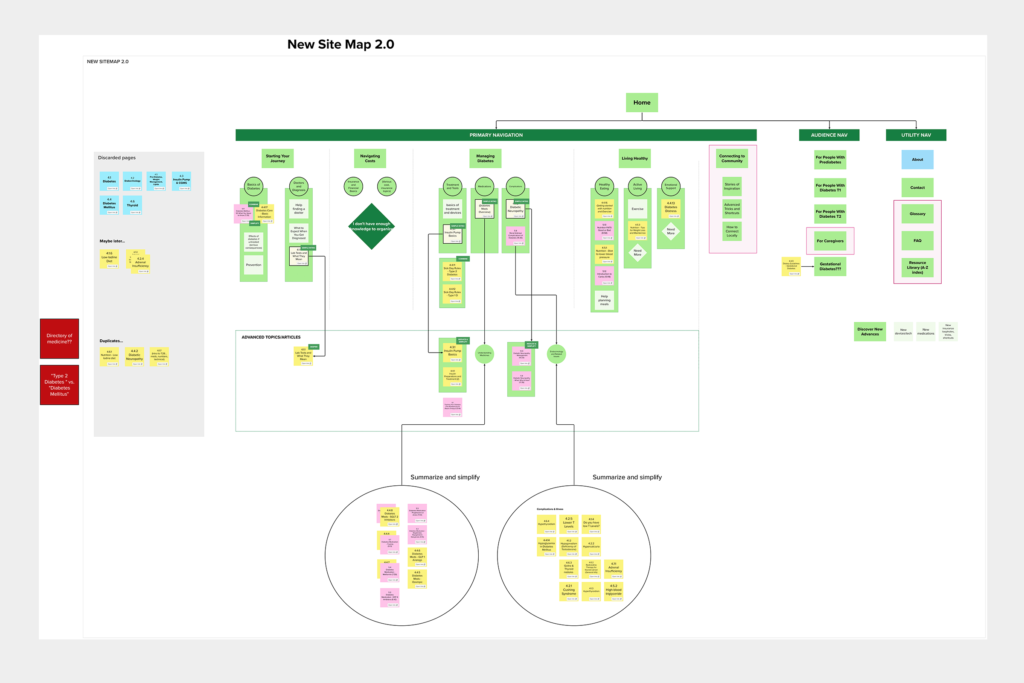
A new sitemap
Usability testing and interview insights served as organizational principles for new IA.
A New Information Architecture
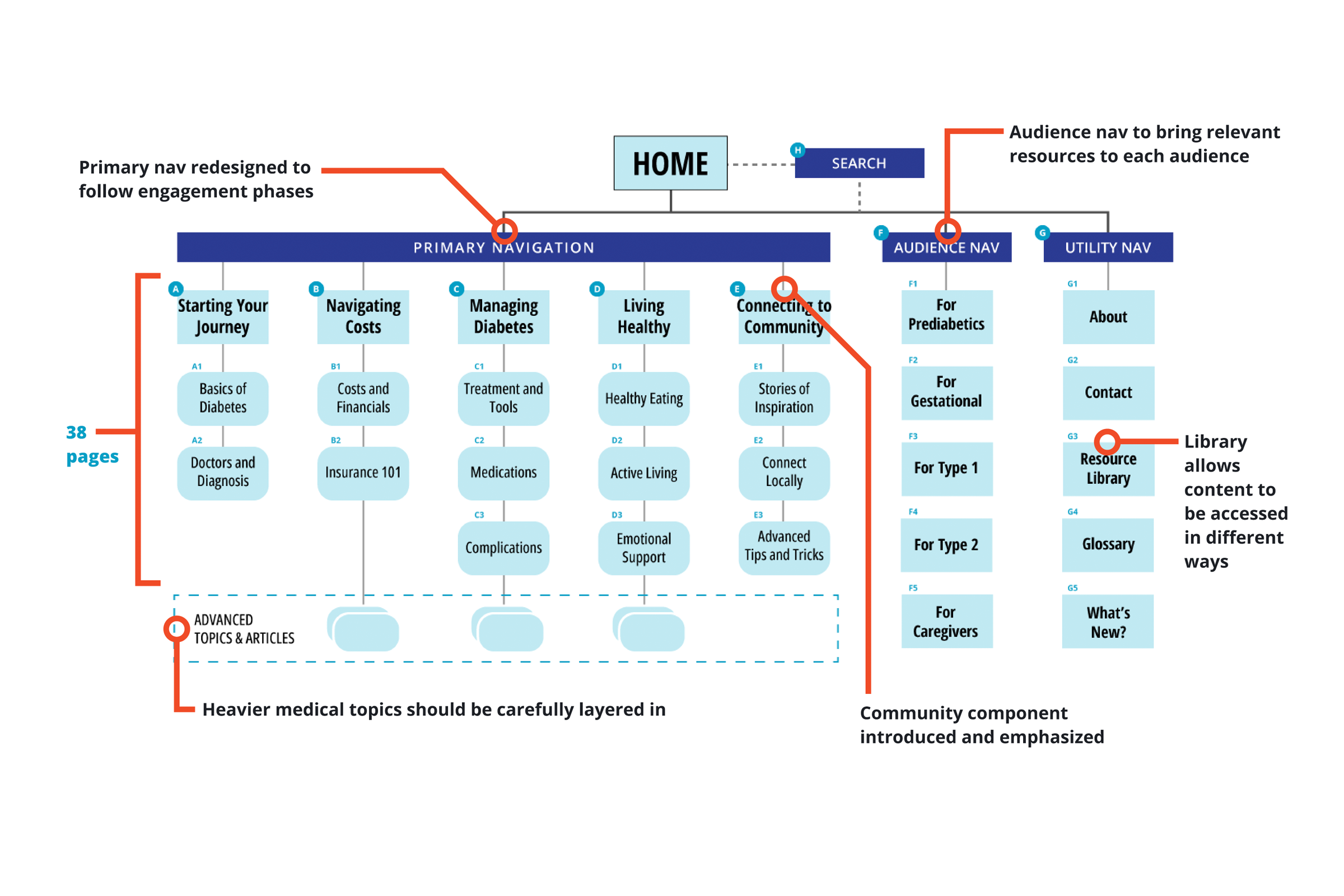
Primary navigation
- The primary nav should be redesigned to follow the engagement phases
- The site would be streamlined to only 38 pages
- Heavier medical topics would be carefully layered in
- We recommend adding a community component
Audience navigation
- This new feature would allow for the aggregation and curation of content depending on who the user is:
- People with pre-diabetes
- People with gestational diabetes
- People with type 1 diabetes
- People with type 2 diabetes
- People who are caregivers to those with diabetes
Utility navigation
- Meant for the general/about pages of the website
- A resource library would serve as an overall index of the site and its topics, showcasing content in different formats
- A glossary would help users quickly refer to any word or topic they might not know, since there is so much technical language with diabetes
Conclusion
Branding, Content & Multimedia
This last section covers the strategies and foundational frameworks crafted by the other teams.
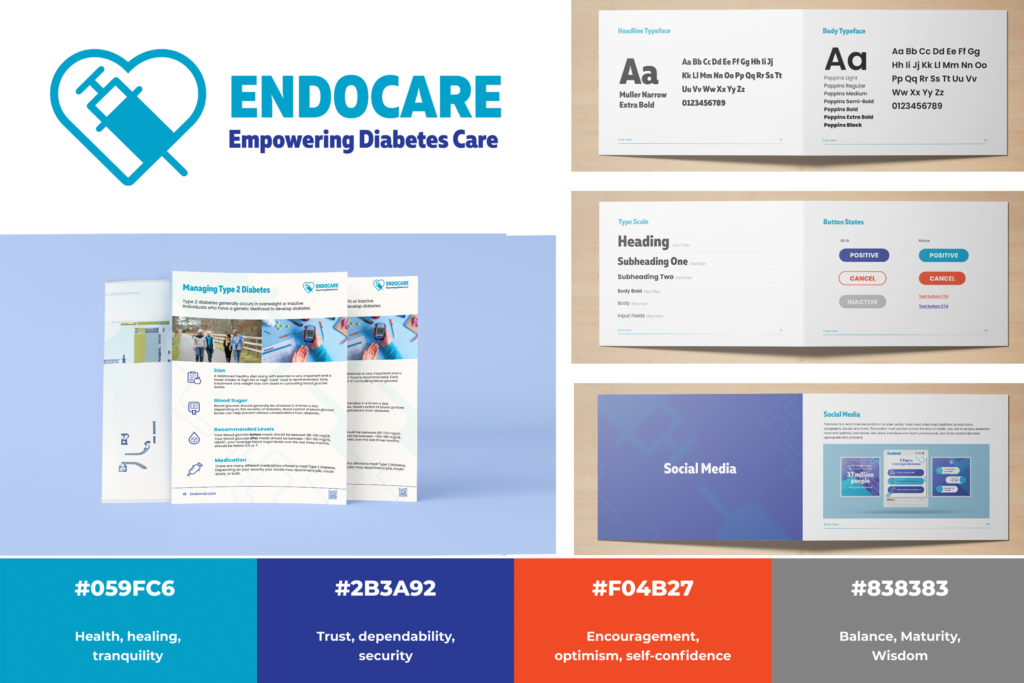
Branding Strategy
The brand team established a trustworthy and memorable brand identity centered around healthcare and diabetes management. This was achieved by utilizing recognizable healthcare-related colors, a logo featuring a depiction of a syringe, clear typography, and designing with a senior-friendly approach in mind.
Based on: build trust, clarify, and encompass.
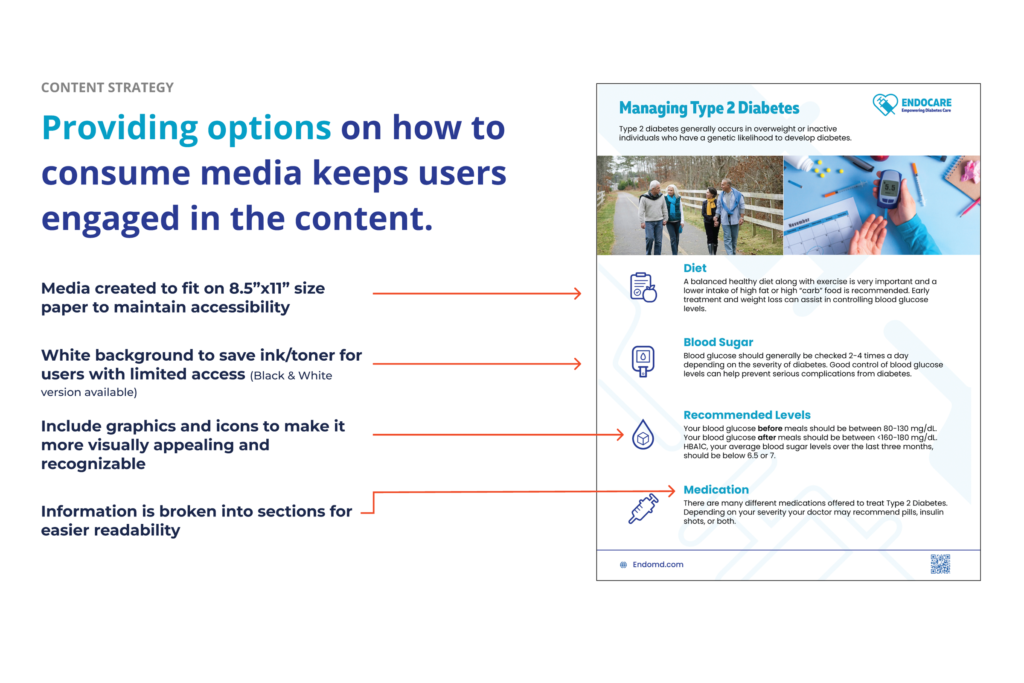
Content Strategy
The content team executed primary and secondary research to build accessible content that addressed the unique needs of rural populations.
Based on: build trust, clarify, and encompass.
Multimedia Strategy
The multimedia team explored elevating educational content through short videos. Their aim was to increase engagement and retention, accommodate for visual and auditory learning styles, and build trust with audiences.
Based on: educate, clarify, and build trust.
Next Steps and Handoffs
This team has set the groundwork for the future research and design work that is yet to come. We provide a proposed plan for how this work could continue.
The building blocks could help drive design decisions moving forward. The evolution of this service design should try to:
- Educate
- Clarify
- Encompass
- Build trust
- Lead with empathic care
While the list is not exhaustive, using the metaphor of building blocks creates a versatile system of design principles that can be removed, replaced, stacked, and arranged in multiple ways.